 |
| Brandy and her 7th baby postpartum Notice the large central IV line in her neck and IV line in her arm for quick blood transfusion |
As part of Cesarean Awareness Month, we are drawing attention to the high cesarean rate and the public health implications of too many cesareans.
One of the complications of multiple cesareans is that the placenta in a subsequent pregnancy can implant too low in the uterus (placenta previa) or grow into the uterine wall (placenta accreta).
This can cause life-threatening complications, including premature birth, impaired growth, or stillbirth for the baby, and severe hemorrhage, hysterectomy, and even death for the mother. Placental abruption (placenta detaching too early) is another potential risk after a prior cesarean.
We've written about placental complications after cesarean before. As a brief reminder, there are three levels of severity in accretas:
- Accreta (placenta is abnormally attached to uterus and can't detach easily after birth)
- Increta (placenta grows into the wall of the uterus and cannot detach after birth)
- Percreta (placenta grown through the wall of the uterus and into surrounding organs)
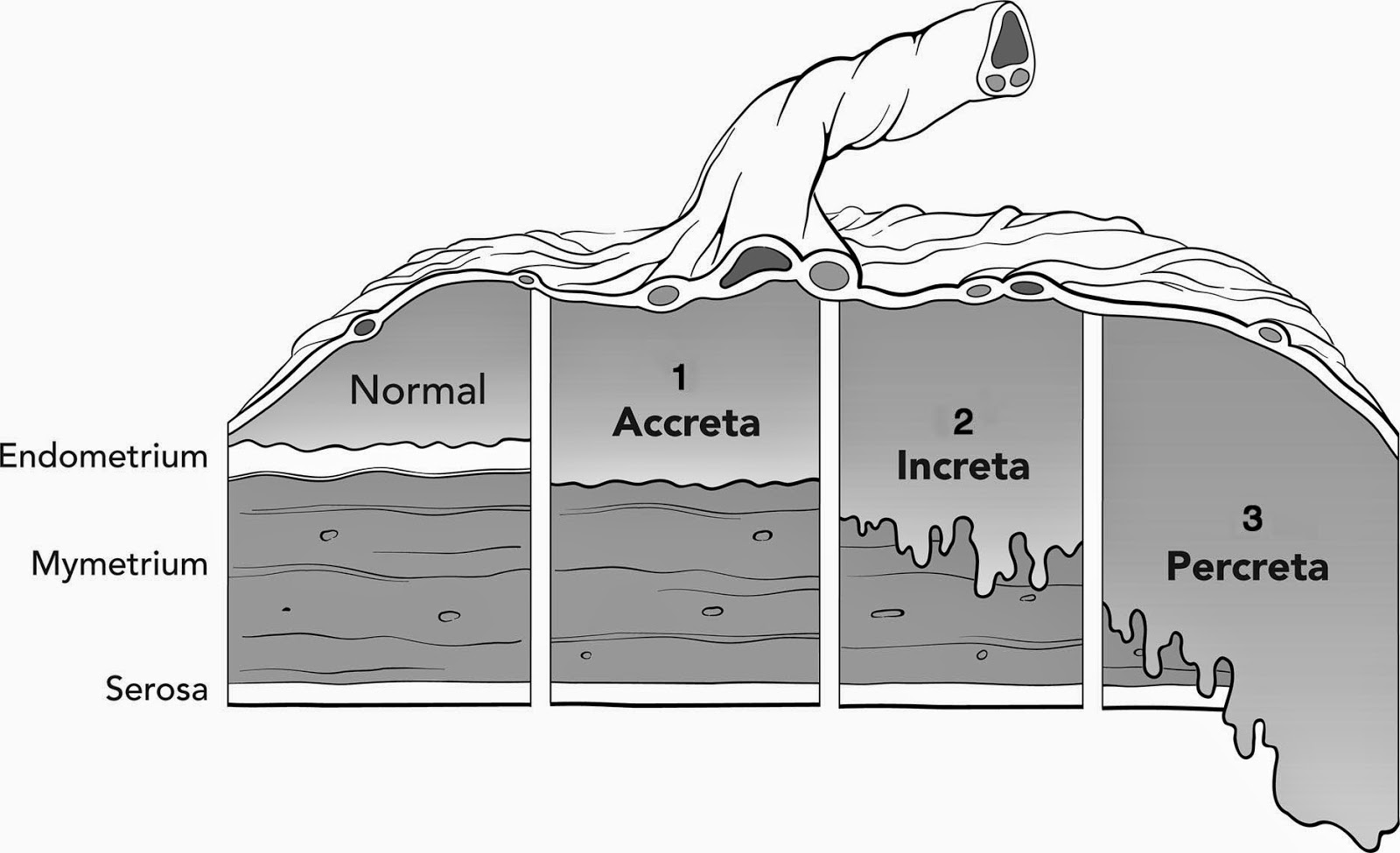 |
| Image Source: Reitman 2011, Anesthesiology |
[If you are looking for more technical information about placenta accreta, see Part One (what is accreta, how a placenta works), Part Two (risk factors, symptoms, and incidence of accreta), Part Three (risks to mother, baby, and future pregnancies), and Part Four (diagnosis and treatment) of my prior series on placenta accreta.]
This time, rather than writing about what accreta is and how to manage it, we present the first-hand story of one mother's experience with placenta accreta (increta in her case).
It's important to remember that placenta accreta is real and affects real women and babies. Do enough cesareans, and increasing numbers of women will face this devastating and life-threatening complication. I've known several women now who have been affected by this condition; all suffered severe hemorrhages and several lost their fertility and uteri forever. One lost her baby and very nearly her life too.
That's why it's so important to do cesareans only when medically indicated and to keep VBAC (Vaginal Birth After Cesarean) an option for those who want it.
Brandy's Story
Brandy has had 7 births and 2 miscarriages. 3 of her births were by cesarean.
Yes, high parity is a risk factor for placental complications, but multiple cesareans is a stronger risk factor. Combine the two and the risks multiply.
Her first birth was a c-section after mismanagement by her doctor. She was told she'd never deliver a baby over 8 lbs. and that her babies were "too big" for her to deliver vaginally. She developed a terrible infection and wasn't allowed to hold her baby for 3 days.
Her second birth was a VBAC at 32 weeks. The placenta detached prematurely and baby might have had some lack of oxygen issues. He passed away at 21 months from seizures.
She miscarried her next pregnancy. Her third birth was another VBAC. She had to fight hard for it when her labor stalled for a little while but in the end she had a VBAC.
Her fourth birth was a CBAC (Cesarean Birth After Cesarean). She had a big baby (10 lbs.) and her doctor scared her into a repeat cesarean because of a recent shoulder dystocia in the practice.
Her fifth birth was another CBAC. Her doctor was opposed to a VBA2C. After her water broke and labor did not start for several days, she had the repeat cesarean. The doctor said she had very little scarring and could have more children. The risks of multiple cesareans, including accreta, were never mentioned.
In her next pregnancy, Brandy weighed the potential risks of VBAC after multiple cesareans against the cumulative risks of multiple cesareans and chose VBAC. She stayed at home in order to have a supportive provider. Her sixth baby was a homebirth VBA3C. He was 11 lbs. 4 oz., three lbs. bigger than her first doctor said she could ever birth vaginally.
She had another miscarriage again, then became pregnant a few months later. She planned another VBAC. Unfortunately, this time the fertilized egg implanted low, near the cervix (placenta previa) and the placenta grew into the uterine wall and into the cervix itself (placenta increta).
In the end she lost her uterus and most of her cervix and suffered a severe hemorrhage but was very fortunate to escape with her baby and her life.
This is the story of Brandy's placenta accreta pregnancy and birth.
I was so excited when
I found out I was pregnant. I was also very scared since I had just miscarried
8 months prior. At 7 weeks when I
started spotting I just knew something was wrong. I had no idea what the real
problem was and what I would end up facing.
I decided to go to the ER and get checked. It was a pleasant
surprise to see a healthy little heart beat. I did notice on my discharge paper
that it was noted that the placenta had attached to the lower uterine segment.
A week went by and I was still spotting. I called my OB and
they decided to schedule a ultrasound to check on things. The ultrasound tech
noted that I had a short cervical length. I was sent to a perinatologist to see
if they wanted to place a stitch. I was very confused. I had already carried 6
other children. I did deliver one of my babies at 32 weeks, but I never had a
incompetent cervix.
The perinatologist quickly pointed out that I had a complete
posterior placenta previa. I was so upset; I knew that would mean another
c-section. I had already had 3 c-sections; I did not want another. I had already
begun dreaming of another beautiful HBA3C. I had it in my head how I was gonna
make a music list and dance through labor. I was gonna walk around outside in
the nice cool October weather. I was looking forward to feeling every
contraction and being more relaxed this time since it would be my 2nd
HBA3C. [kmom note: Home Birth After 3 Cesareans]
Time went on and I continued to get ultrasounds monthly. It
was always the same thing...the placenta had not moved. I was still spotting everyday; it was there every time I wiped. At one ultrasound appointment my OB made a
comment that she saw a lot of placental lakes. I started researching placental lakes and learned that they are seen a whole lot with accreta. I started to
worry.
I finally got good news at my 20 week ultrasound. The
perinatologist said it looked like the placenta had moved and it was only the
tip of it covering my cervix. He did say that there was a blood clot covering
the cervix now, but that my body should reabsorb it. I questioned him a little
bit about the blood clot. He reminded me that I had been spotting and that is
what it was from. I had noticed the spotting had been slowing down so it all
made sense. It was good news! The placenta moved some and I had a healthy baby
boy. No one had to tell me I was having a boy; he decided to show off for momma.
I left the doctor's office practically skipping. I went and
bought a bunch of "It's a Boy" balloons and filled a bag with them to let my other
kids tear open. We were all so happy and back to planning our home birth.
At the next ultrasound I was 24 weeks and I just knew they
were gonna tell me the placenta had moved more.
The look on the ultrasound tech's face said something was wrong. When she
told me she wanted the doctor to see it I felt my stomach go into my throat.
Two
minutes felt like a century as the doctor was looking at the ultrasound. He said, “What I believed was a blood clot last appointment actually looks like a
accreta.” He then went on to say that unfortunately with your c-section history
and what this looks like, it I am pretty sure we will have to take your womb.
He went on to show me how vascular one section of the uterus was. He continued
to talk about unfortunately this is like the weather, there is nothing you can
do about it. He continued to talk and all I heard was some mumble about any OB
can do a hysterectomy and I should be able to deliver at my local hospital.
I was numb, how could
this be. I waited at the check-out desk trying to breathe, trying not to cry. I
got my card for my next appointment as the tears started to fall. I don’t know
how I walked to my car. My phone rang and I could not get out hello.
After I had a little while to process things and talk to a
few people I decided to go to get a second opinion in Baltimore. The blood clot
theory made sense. My spotting stopped at 22 weeks. I figured that was a good sign. The
specialist in Baltimore knew more about accreta and could give me better
answers.
Once I got to my appointment in Baltimore, that look the
first tech had, I saw it all over again. This look of fear, maybe even
confusion, just like the tech before she went to go get the doctor. He showed me that the placenta was supposed
to look black on the ultrasound and there was these weird gray areas. He told
me that at the least we were dealing with increta, but that he believed it was
percreta.
He went on to say all my care would be transferred there. That with
this condition there would be massive blood loss and my local hospital could
not handle delivering me. I tried to be strong but I burst into tears. We
decided to do a MRI to try to get a better ideal if any of my other organs were
involved.
Everything then just became a blur. I spent every Monday in
Baltimore seeing doctors and having ultrasounds. The group of specialist were
waiting on the MRI results to decide whether to deliver closer to 34 or 36
weeks.
Once the MRI results
came back it looked like no other organs were involved but that the placenta
was invading the uterine wall. I was so happy to get the news that none of my
other organs were involved. That was the first time through all of this I got
good news. It is funny looking back now how wonderful that news really was to
me. Since I was doing good and had no
bleeds they decided to schedule my c-section at 36 weeks. Some of the doctors
were still hopeful that once they got in there the placenta would detach
easily.
I had 6 weeks until delivery and I was trying to understand
and accept things. I was terrified. I felt like a ticking time bomb. I could
not sleep. My husband was working nights so I was alone with 4 little ones,
eight and under. I was scared I would have a bleed in the middle of the night
and the kids would be terrified. When I did sleep I would have nightmares of
having a c- section and my incision opening up and I was standing there holding
my insides.
I would hold my little ones and wonder if I would be able to see them grow up. I would
think, "My 2 year-old will not remember me." I think all these thoughts but had no
patience with my kids. Then I would think if I don’t make it all they will
remember is me snapping at them.
One of the hardest things I had to deal with
was knowing that the people that got me here by doing 3 unnecessary c-sections
on me were the same people I now had to trust to get me out of this.
As the weeks went by I realized that I had no control over
the outcome. I had to do the best I could and control what I could and give the
rest to God. I had to believe that even
if I did not make it through that God would take care of my kids and it would
be OK.
Days before my delivery I had to go do pre-op blood work
and meet with anesthesia. I was told with the blood loss they were expecting I
may have a lot of swelling and fluid in my lungs. They may have to keep me
asleep until Friday until the swelling went down. They wanted my family to be
prepared. That broke my heart to think I may not see my baby on the day he was
born. They said I would go home with a bladder bag if they had to do the
hysterectomy. With the scar tissue from my c-section they were sure that
they would rip my bladder when they removed my uterus.
Delivery day came saying good bye to my kids was one of the
hardest things I ever had to do. They were so excited to meet their brother the
next day. And I had no idea if I would ever meet my baby or see my other kids
again.
I got to the hospital around midnight. They got me situated
in my room and then let me sleep for a few hours. I would doze off for a few
minutes then wake back up with a knot in my stomach and a lump in my throat. I didn't want to be there. I wanted to run far far away from that place.
At 6 a.m. they came in and started to get me prepped for
surgery. We had decided that it was best for me to just be put under general.
My surgeon was afraid he would lose time if I began to hemorrhage and they had
to put me under then. They did not want
the baby to be under general any longer then he had to.
All the prep was done in my room. Anesthesia
came and placed a central line in my neck and a large IV in my wrist; both of
those were for blood transfusion. They also placed a monitor in my wrist that
would send labs and gives them second-by-second blood pressure reading. By this
time I was numb, I had shut down. I just prayed and sang worship songs in my
head and took myself away from there.
My surgeon came in and did a quick ultrasound to see where
he was gonna cut. As funny as it sounds
I was still hoping that he was gonna find that the placenta had moved.
Once it was time to go to the OR the two main surgeons
wheeled me down. My husband got off on another floor to wait in the waiting
room. I just wanted to scream, “NO!” I didn't want my husband to go. I wanted
him there when I fell asleep. I just gave him a kiss and told him I will see you
in little while. He said a quick prayer and slipped off the elevator.
We were outside the O.R. doors and had to wait. The blood bank
had not brought down the blood that was to be on stand-by in the O.R. There were doctors everywhere. My neck hurt so bad from the central line. I could barely
move. And there was so many people coming up introducing themselves. MY nurse
kept saying, “Oh my goodness, everyone is here.” She said, "You have the best of
the best!"
All of a sudden here comes two big coolers. I just hear everyone say,
“OK, let's go.” My surgeon told me, "I have been resting for 2 days for your
surgery."
I said, “Hey, you have to take good care of me. I have lots of little
ones that need me.” He said, “Brandy, we know what you got and we are gonna take
good care of you.”
Things got real busy in the O.R., they put the oxygen mask on
me, and kept telling me to to take nice slow breaths. The mask made me feel
like I could not breathe. I was getting frustrated that I was not asleep yet. I
wanted it over. No matter what the outcome was gonna be I was ready to get
there. Everyone was rubbing my arms telling me that they were there and they
aren't gonna leave, that I was OK. I remember thinking I am never gonna fall
asleep.
I heard, "Don’t talk, you still have the breathing tube in." I
raised my arm and started to write in the air. The nurse got me a paper and
pen. I wrote "b" and dozed off, I wrote "a" and dozed off. The nurse said, "Are you
writing 'baby'?" and I shook my head yes! She told me that he was healthy, 7lbs 2.5
oz. He had no problems and went straight to the newborn nursery.
They took the breathing tube out and I said, "Is it Friday?" and
the nurse said, "No, it is Thursday, 2 in the afternoon!" I was so so happy my baby
was OK and I was still here. It was finally over! The worry, the fear, the
unknown!
My surgeon came and held my hand and told me that they did have to do the
hysterectomy, the main vein in the placenta had grew very deep into my cervix.
They also had to take most of my cervix. I lost 7 ½ liters of blood. I was
given 13 units of blood products.
[kmom note: 7.5 L is 7500 ml. Normal blood loss in a vaginal birth is 500 ml; 1000 in a cesarean. She had more than 7x the normal blood loss for a cesarean.]
[kmom note: 7.5 L is 7500 ml. Normal blood loss in a vaginal birth is 500 ml; 1000 in a cesarean. She had more than 7x the normal blood loss for a cesarean.]

I didn't care at that point. I was alive, my baby was healthy! We made it to the other side. PRAISE GOD we were OK!
I met my little man when he was 8 hours old. He is perfect.
I would do it all again to have him. We have both done very well recovering
physically. I didn't need a bladder bag after all. I delivered on a Thursday
and we came home together on Sunday.
But emotionally it has not been so easy. I do sit here in
disbelief sometimes wondering why me? Other days I get angry. I want to punch
something and yell GIVE ME MY UTERUS BACK! I mourn the loss of my fertility,
the loss of his birth and the first 8 hours of his life. The loss of my last
pregnancy. The loss of some relationships that have been damaged through all this
for one reason or another.
I share my story not
to scare anyone. I know what it feels like to be scared into something. I would
never want to do that to someone else. I just want women to be aware of all
possible complications. I want women to be able to give true consent and be
aware of all risks.
If sharing my story saves one women from having a different
ending than me then it wasn't all for nothing. Accreta is not talked about, but it is real, very real!

